The following content is from a tri-fold pamphlet created by plastic surgeon Douglas Ousterhout in 1994 and mailed to prospective patients. The content was initially transcribed, scanned, and published online with additions by Ousterhout patient Heather Jean Lamborn of heathers.net. Ousterhout patient Rebecca Allison of drbecky.com then published a version without embellishments. On its 25th anniversary, this highly influential document was prepared and published by Ousterhout patient Andrea James at transgendermap.com for historical interest.
Feminization of the Transsexual
Douglas K. Ousterhout, M.D., D.D.S.
Looking feminine is, of course, extremely important to you. First impressions are often based just upon your face. That which is first seen in an initial contact is frequently what defines you. It establishes not only who you are, but often what sex you are as well. As a transsexual, perhaps nothing is more important to you than appearing sexually the same as you feel emotionally. Facial feminizing surgery can help bring these two together.
Cosmetic (aesthetic surgery) of the face can be directed toward many aspects of facial appearance. The majority of facial aesthetic surgery in this country is to reduce the effects of aging – reducing wrinkles, lifting sagging skin, or removing fat deposits. Facelifts, brow (forehead) lifts, blepharoplasties (cosmetic surgery of the eyelids), and removing excess fat in the neck are among the most frequently completed aesthetic facial soft tissue procedures that I do. A great deal of my aesthetic surgery, though, is directed toward changing facial contours by modifying the basic bony supporting configuration of the face.
Surgery such as a rhinoplasty (nasal surgery), chin, cheek and forehead modifications (either reduction or augmentation), changing the shape of the mandibular angle, and – in certain patients – moving the upper and/or lower jaws are frequently completed by me as well.
I have edited the only medical book describing all of these different types of bony surgery that can be completed on the face. This book, titled Aesthetic Contouring of the Craniofacial Skeleton (Little, Brown and Company), also discusses another important aspect of facial contouring – Feminization of the Face.
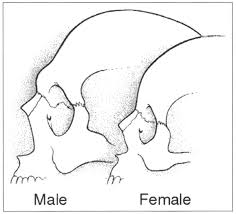
There are basic differences between a male and a female skull – differences long appreciated not only by anthropologists studying skulls, but by artists as well. Females have a more pointed chin and less nasal prominence than males. The forehead is quite different, especially the areas of the brows and the mid forehead. The shape of the skull affects the drape and contour of the skin. Changing the shape of the skull will assist in changing one from distinctly male to female. Modifying the angle of the lower jaw and the prominence of the cheeks can also help improve femininity.
The techniques used and the areas modified are individualized. Quite obviously some transsexuals are already much more feminine than others. What is completed is based upon a combination of skeletal and artistic evaluations, radiographs (x-rays), anthropological measurements, asymmetry gauges, facial masks and photographs. Patient self assessment is also very important to surgical planning. Based on all of the above, a treatment program is established.
The following is directed at various aspects of the surgical recontouring. Finally, there is a brief resume about me as your surgeon.
OBJECTIVE
My main objective in this surgery is to make you as feminine as possible, in order for you to be as comfortable as possible in your new direction. When the surgery is completed, we want you to be seen as a female. Most, if not all, of our transsexual patients are very happy with the surgery I have done for them.
We are also happy to work with those who wish to be feminized, to any degree, but are not planning on genital reassignment surgery. Please do not hesitate to call or write us to ask for our assistance. You will find my staff to be most helpful and confidential.
EVALUATION
During the initial consultation, I will evaluate your health, complete an appropriate examination, make essential measurements, obtain photographs, and order the appropriate radiographs. I will then ask you to return for a more extensive discussion of my suggestions for your feminization. There is no additional cost for the second or any other additional office visits. After we have completed a discussion on what would be the most helpful to you (i.e., any operation(s) and their purpose), I will review with you the surgical procedures. If there is more than one procedure being recommended, we can discuss what procedures can be completed together, potential complications, recovery time, and costs. Before you will be scheduled for any surgery, it is hoped (if you are a transsexual) that you would have seen, and be under treatment by, a psychologist or psychiatrist and a medical internist or endocrinologist.
SURGICAL PROCEDURES
FOREHEAD
The forehead covers a very large portion of the face. As the male forehead is so different than the female forehead, this may be one of the most important areas to modify. Males have brow bossing, with a flat area in-between the bossing, while females tend to have a completely convex skull in all planes. Based on differences in anthropological measurements, the size of the frontal sinuses (in the mid lower forehead above the nose and eyes), and the general contour of the orbits and forehead, three different ways to modify the forehead shape have been developed. This varies from bony contouring to the most involved procedure, in which the anterior wall of the frontal sinus is placed into a more posterior position. Orbital rim contouring may be necessary, and will be completed at the same time. A forehead lift can also be accomplished during the same operation, if indicated. The surgical approach to these various procedures is all basically the same, i.e., an incision in the scalp, either within the hair bearing area or in front of the hair, as indicated for each individual.
SCALP ADVANCEMENT AND BROW POSITION
In physical anthropology studies, it has been shown that men have a longer distance from the brows to the hairline than do women. This is true even without any evidence of male hair loss. The average for women is approximately 5.0 centimeters (2.0 inches), as opposed to men’s 7.0 centimeters (2.6 inches). In actuality, I find that in the majority of the transsexuals that I see this distance is actually between 7 to 8 centimeters (2.7 to 3.1 inches). A long forehead is generally acceptable for the male, but not for the female. Women with long foreheads will generally either wear bangs or will comb their hair in a way such as to hide some of their forehead. Small hairpieces are also used. This routine is not a decision based on forehead length, but rather the finding by women that they just “look better” with their hair farther down on their forehead. Women with long foreheads rarely wear their hair back as in a ponytail.
In general, we like the position of the brows in the female to be higher – over the superorbital rims – while in men it is quite normal to have the brows slightly under the supraorbital rims. In fact, if they are higher in the male – like in a female – they may look surprised or effeminate. Elevation of the brows can be nicely completed in a standard forehead lift. This is also routinely completed in the forehead feminizing procedures.
Combining the forehead bony feminization, brow lifting, and scalp advancement, has for years been a very concerning problem; the fear being that the scalp would pull back farther, thus elevating the brows into a very abnormal position and causing the appearance of extreme surprise. I have developed a method whereby both procedures can be completed simultaneously with excellent results. This has now been completed in many patients, both male and female. The net result of this procedure in the MTF transsexual who has this particular hairline and forehead length, is considerable feminization.
Forehead and/or scalp advancement are generally completed under general anesthesia, but can be completed under local anesthesia and sedation (in selected cases). The procedures are completed through an incision just at the hairline in the middle two thirds of the forehead, and then extend laterally more posteriorly into the hair and down to the superio-posterior of each ear. The prehairline scar heals very nicely, but, depending upon ones preferred hairstyle and the quality of the healed scar, may benefit from a few micro hair grafts in front of the scar. As you probably know, the male hair pattern is generally nicely maintained while on female hormones.
RECOVERING FROM FOREHEAD SURGERY
This surgery is generally completed on an inpatient basis, and most patients will spend one night in the hospital following surgery. A dressing is placed around the forehead after surgery, and left in place during the first night. It can be removed the day following surgery.
After removal of the dressing, showering and gentle washing of the hair is completed daily for a few days. If chin surgery has been completed at the same time, there will be a tape supporting dressing. This must stay dry, in which case the hair will need to be washed by someone else while lying down.
There will be some pain for a few days, which will require some pain medications. While infections are extremely rare, antibiotics are utilized to avoid any potential infection. Swelling and any black and blueness that occurs around the eye will generally be gone within ten to twelve days following the surgery. There may be some forehead numbness lasting several weeks to possibly years. Other nerve injuries that might rarely occur will be discussed.
Many patients are able to go back to work at their usual activities (especially if they can work at home) within two to four days following surgery. It is not advisable to do anything that would require exertion sufficient to cause you to sweat or to have a rise in pulse or blood pressure for eight days following surgery. The sutures and staples utilized to close the scalp incisions are generally removed by nine days following surgery.
The results from this portion of the surgery are generally very dramatic, and offer tremendous psychological support.
CHEEK SURGERY
While the shape of the cheeks and their prominence, or lack of it, is not generally a female or male characteristic, it is true that a lack of cheek prominence is often not appealing. In particular, it is very pleasing for a female to have full but not overly prominent cheeks. Augmentation is, therefore, often very helpful in feminizing the face. Cheek reduction can be completed, but is a much more rare need and, as such, will not be discussed here.
Cheek augmentations are generally completed utilizing an implant, but certain bone cuts and bone segment repositionings are useful in selected individuals. Various sizes and thickness of implants are available to fit individual differences and desires. The implants are most often placed with the patient under sedation and utilizing local anesthesia. The approach is usually through the mouth so no skin incisions are necessary. Rarely are implants placed through a lower eyelid incision. The implants are placed through a tunnel, into a pocket under the soft tissues, and immediately overlying the cheek bones. The sutures dissolve and go away on their own. In general, I do not like “submalar” implants.
RECOVERING FROM CHEEK SURGERY
There is usually a moderate amount of swelling following the placement of implants. Pain medication will be necessary. Because the implant is a foreign material and is being placed through the mouth, antibiotics are utilized to prevent the possibility of infection. If an infection were to develop in spite of antibiotics, the implants might have to be removed. Because of some temporary numbness that may occur, and because of stiffness in the cheeks secondary to swelling, speaking and smiling sometimes seems interfered with for a while. Yawning and chewing may feel funny. These abnormal sensations generally pass within a few days following the operation. Some of the porous implant materials, such as Medpor, seem to cause more temporary swelling than silicone, but the swelling is generally gone within a couple of weeks following surgery. The swelling is not so great as to interfere with normal functioning. It is generally advisable to avoid foods requiring a great deal of biting or chewing. Tooth brushing will not be interfered with, but one needs to be careful for there will be some tenderness around the incision line above the teeth.
NOSE SURGERY
The nose
varies tremendously from individual to individual and, of course, may be quite
masculine compared with being desirably female. If one has thin skin, a
significant size reduction can generally be completed. If the skin is quite
thick (as is often the case in males), the contour can still be markedly
improved, but there may be a definite limitation to the size reduction
possible. However, contour changing alone greatly feminizes the basic nasal
appearance. If there happens to be a breathing difficulty coexisting with an
appearance deformity, these can often be improved markedly by the same surgery.
Nasal surgery is usually completed under general anesthesia, and requires one
night in the hospital followed by ten to twelve days for more complete recovery.
CHIN SURGERY
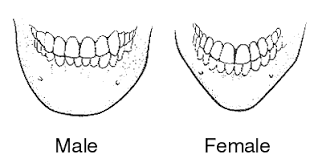
The chin varies markedly between the male and female. The male chin is generally wide and vertically high, while the female chin tends to be more pointed, narrow, and vertically shorter. The degree of masculinity/femininity can vary tremendously. The chin, therefore, is an extremely important area in gender recognition.
The chin can be modified in numerous ways, both to improve facial appearance and to feminize the lower face. It may require only a small implant, or possibly extensive bony cuts and repositioning of the chin. Various modifications to the chin can be made depending upon the individual anatomy of the patient, and the desired end result.
Occasionally, even with the bony osteotomies, various types of implants are additionally necessary to obtain the desired contour. As the surgery necessary can vary tremendously, the costs will also vary, One can, however, state with fair confidence that anything that one wants to obtain with a chin can be accomplished. This is, of course, somewhat of an exaggeration, but it is an extremely modifiable area.
RECOVERY FROM CHIN SURGERY
The recovery time varies with the amount of surgery being completed. With an implant the recovery time may be only two or three days, while a very extensive bony procedure may require as much as four to five weeks for healing to be quite complete. Even in the more extensive procedures, one can usually return to their usual activities, except for heavy exercise, within five to six days of surgery.
ANGLE OF THE MANDIBLE SURGERY
Males tend to have a more obvious mandibular angle, with thicker muscles and resulting fullness, than does the female. The contour in the male is usually due to a heavy masseter muscle and, as a result, a lateral and posterior flaring of the bony angle occurs. The female tends to have a smaller muscle and more of a gradual curve, or even a straight line, along the lateral border from the posterior border of the mandible to the chin area.
The lateral border of the male mandible may be very full and round, adding to the squareness of the lower face. This gives the male a heavier, fuller looking lower face, while the female has a narrower, more tapered face in all aspects.
Modification of the lower face can reduce some of the obvious aspects of masculinity, and create an improved feminine appearance. The lower jaw contouring procedure is completed through incisions in the mouth, while under general anesthesia. No skin incisions are made. The masseter muscle is reduced on its internal surface, i.e., the portion adjacent to the bone. The bone is then further reduced laterally, as well as softening the bony angle.
This surgery usually takes approximately three and a half hours while under general anesthesia. You generally must stay in the hospital one night following the operation. The face will become moderately swollen and somewhat black and blue following this surgery.
Recovery is consistent with the other procedures – that is, you can return to your usual activities in eight or nine days following this surgery. The final result, however, will not be seen for many weeks, as it takes at least four to six weeks for the improved contour to become totally obvious. Most patients are quite comfortable going back to work a week and a half to two weeks following the surgery.
THYROID CARTILAGE REDUCTION (ADAM’S APPLE)
Reducing the size of the thyroid cartilage, the upper portion of which is the Adam’s Apple, is almost imperative in feminization. To have a female facial appearance and an “Adam’s Apple” is a sure giveaway of ones sexual origin. The cartilage is reduced through a small transverse incision in the neck immediately overlying the cartilage prominence. After the cartilage is reduced, a small amount of steroid is placed in the wound to help keep the scarring to a minimum. While complications from the surgery are few, thick scars occasionally occur, and there have been a few reported cases of undesirable voice change resulting from the operation.
The procedure is usually completed while under general anesthesia, along with one of the other feminizing procedures. It can be completed separately under local anesthesia in special circumstances.
HAIR TRANSPLANTS
Hair transplantation or scalp shifting is very helpful in MTF’s who have considerable, but not excessive, hair balding. There are many ways to improve the female hair pattern. It may require major procedures like a scalp flap, but more often plugs, or small grafts (either macro or micro), are preferable. Scalp reductions are useful in some individuals. On other occasions, tissue expansion can be very helpful for improving the hairline. There are, however, some individuals where baldness is so extensive that there is no choice but to use a hairpiece. Like all of the procedures described in this brochure, individualization is a must. Obviously, the results will depend upon the individual’s basic hair appearance, combined with the results from hormones and associated surgical techniques.
BREAST AUGMENTATION
The individual breast development response to feminizing hormones, in most transsexuals, is one of mild to moderate breast development. In some individuals this is quite satisfactory, while in others a greater fullness is desired. If a larger size is desired, breast augmentation is possible utilizing various implants and techniques. This must be individualized through consideration of patient desires, physical contours, and physician philosophy. No attempt will be made to discuss these issues at this time. Rather, let it be appreciated that the results are generally very pleasing – especially when the response to hormones has created some breast thickness, as this will usually very nicely hide the implants.
Augmentation can be completed under either general or local anesthesia. The procedure takes approximately two and one-half hours, and is completed on an out patient basis. It may be combined with other surgical procedures. Drains are usually left in for one to four days. Most patients are quite comfortable within three to five days following the operation, and require very little pain medication.
At the present time, utilizing textured saline filled implants, the breasts are fairly firm for the first three to six months, and then begin to soften. The softening process may take several more months, but when completed offers a very pleasing result. Capsular contracture, which causes an artificial round appearance, is unusual with the new prosthesis.
Breast augmentation has always been one of the happiest operations that we do for our female patients. The same is true for my MTF patients as well.
BODY CONTOURING: ABDOMINOPLASTY & TRUNK CONTOURING (WITH SUCTION ASSISTED LIPECTOMY)
For completion of overall effect, body contouring may be very important. Abdominoplasty (tummy tuck) by suction assisted lipectomy or surgical assisted excision will greatly improve ones lower trunk contour, with the incision and resulting scar placed low on the abdomen, just above the groin. By lateral narrowing (muscle plication), the abdominal shape can be markedly improved towards a feminine contour. The waist line can be reduced. While abdominal femininity can generally be improved, the overall results will greatly be affected by one’s overall size and total body weight (obesity).
I personally do not recommend lower rib excision, as the scars at the excision site are bad, and the ribs generally redevelop. The body needs the ribs for breathing and, with rare exception, will redevelop. The improved contouring from rib excision is generally not maintained.
Hip, thigh, and leg suctioning can be completed to facilitate reduction contouring. How much can be completed depends upon body size and shape, as well as the amount of obesity. It is difficult in this short text to go into much detail regarding the pros, cons, and potential of such procedures. Patient consultation will absolutely be necessary for individualization.
Many patients desire to have wider hips or fuller buttocks. I am often asked about fat injections and implant placement. While the surgeries can be completed, the results are not generally pleasing. Fat injections are, contrary to lay medical reports in various magazines, not satisfactory. There is excessive and irregular absorption of the fat. The results are generally temporary at best, irregular and asymmetrical at worst.
Implants
are often very uncomfortable to sit on if placed in the buttocks. Elsewhere,
subcutaneous implants (other than under the breasts and on the face) look like
implants under the skin – obvious in appearance and nonfunctional in their
movement. I do not recommend their use.
ADDITIONAL SURGICAL PROCEDURES
Soft tissue cosmetic procedures, such as facelift, forehead lift, blepharoplasty, and suction assisted or surgical lipectomy of the neck may add significantly to one’s overall feminine appearance. All of the above surgeries are regularly completed by me. SRS (sex reassignment surgery) or GRS (genital reassignment surgery) is not completed by me but, if desired, I can give you references.
ELECTROLYSIS
I personally do not complete electrolysis, but I can guide you to people who do this. Because electrolysis causes some swelling, facial surgery needs to be appropriately scheduled.
ADDITIONAL BROCHURES
Additional brochures on many surgical procedures are available in our office from such societies as the American Society of Plastic and Reconstructive Surgery, the American Society for Aesthetic Plastic Surgery, and the American Society of Maxillofacial Surgeons. These brochures include: Forehead Lift, Rhinoplasty, Rhytidectomy, Blepharoplasty, Cheek Augmentation, Chin Augmentation, Ear Surgery, Body Fat Reduction, Surgery of Abdomen, Male Body Contouring, Dermabrasion, Facial Implants, Chemical Peel, and Scar Revision. Any of these are available at no cost at your request.
ADDITIONAL CONSULTATIONS
We may also be of help to guide you to various associations, doctors of endocrinology, psychologists, psychiatrists, electrologists, speech therapists, and counselors of various types, who are happy to work with and do work within the transsexual community.
DECISION MAKING
It is, of course, extremely difficult for you to decide exactly how and when to proceed. Working with me, my office staff, and other patients can all be helpful, and we are available to help you make your decision. Photographic results of various procedures completed on other transsexual persons are available in our office. The American Society of Plastic and Reconstructive Surgery also has a financing program available that may be beneficial. We will do everything possible to make your decision in this extremely important matter as easy as possible.
PREPARING FOR SURGERY
I will give you very specific instructions on preparation for surgery, including guidelines on sun exposure, eating, drinking, and avoiding certain medications, such as those containing aspirin, non-steroidal anti-inflammatory drugs such as Ibuprofen or Indocin, or vitamin E.
It is best if you do not smoke for as long as possible before or after surgery, but particularly within a period of one week before through one week afterwards. Smoking interferes with blood supply and can, in certain cases, lend itself to assisting the development of an infection. Also, as some of the facial procedures are done through the mouth, it is important for your oral hygiene to be good, and that you have no obvious infections or sores.
It is necessary to have someone drive you home after surgery, either if your surgery is done on an outpatient basis or even if you stay overnight, . Plan on this.
LOCATION OF SURGERY
The surgery is always completed in an operating room. Those cases that must be performed under a general anesthesia are completed in the main hospital operating room. Smaller, more minor procedures can be completed either in the regular operating room, or in our office operating room. Some of the procedures will require you to stay overnight, while others can be done on an outpatient basis. This will all be discussed with you at the time of your evaluation.
TYPES OF ANESTHESIA
Facial tissue surgery often can be completed under local anesthesia. Cheek implants also can be completed under local anesthesia, but more extensive bony contouring procedures of any part of the face will usually require a general anesthetic. Of course, all of the procedures can be completed under a general anesthetic if that is your desire. Procedures completed under local anesthesia are generally completed with sedation. Under general anesthesia, the patient is completely asleep throughout the surgical procedure. The indicated technique for an individual procedure will be discussed with you.
SCHEDULING
Surgical scheduling is completed by my office staff. They can be reached through my office telephone, (415) 626-2888. In the winter months I am generally scheduled 1-2 months ahead, and about 2-3 months ahead in the summer. If a cancellation were to occur, it is possible that an earlier date could be arranged. We will do everything possible to accommodate your wishes, so please do not hesitate to call us.
DOUGLAS K. OUSTERHOUT, MD
I started my college education at the University of Colorado, Boulder. Next I went to the Minerva Institute in Zurich, Switzerland. I then attended the University of Michigan in Ann Arbor, where I received my dental degree in 1961, and my medical degree in 1965. While there, I was inducted into several honor societies, including Dental Academic, Medical Historical, and Medical Academic Honor Fraternities.
I continued at the University of Michigan as a resident in general surgery after serving as a Captain in the U.S. Army Medical Corps from 1966-1968, and completed my residency in Plastic Surgery at Stanford University Medical Center, where I held the position of Chief Resident from 1971-1972. From there I traveled to Paris to become the first American to assist Doctor Paul Tessier in the techniques of craniofacial surgery.
Upon my return to the United States, I was certified by the American Board of Plastic Surgery in 1974, and have been in the practice of plastic surgery in San Francisco since then. I have fellowships with 185 medical societies including American Society of Plastic and Reconstructive Surgeons, American Society for Aesthetic Plastic Surgery, International Society of Aesthetic Plastic Surgery, Societe Francaise de Chirurgie Plastique Reconstructrice et Esthetique, American Society of Maxillofacial Surgeons, The Harry S. Benjamin International Gender Dysphoria Association, and the International Society of Craniofacial Surgery.
I am, and have been, on the boards of many plastic surgical societies, including being President of the American Society of Maxillofacial Surgeons (1994-1995), and on the editorial board of four different plastic surgery journals. I am on the Advisory Committee for “Recommended Guidelines for Transgender Care”, AEGIS.
I hold staff memberships at several hospitals, including Davies Medical Center, Saint Francis Memorial Hospital, California Pacific Medical Center, and the University of California, San Francisco, where I am a Clinical Professor of Plastic Surgery, participating especially with a panel of experts at the Center for Craniofacial Anomalies. I have operated in many countries outside the United States.
Throughout my career, I have presented dozens of major scientific papers, both nationally and internationally. I have published scores of scientific papers. My recent medical textbook, Aesthetic Contouring of the Craniofacial Skeleton, was published in 1991.
Douglas K. Ousterhout, MD, DDS
45 Castro Street, Suite 150
San Francisco, California 94114
(415) 626-2888
Copyright 1994, 1st Revision 1995 Douglas K. Ousterhout, MD, DDS